Time Out Technique
Contributed by Dr Brown:
Below is a great discussion on the "Time Out" Technique to control for difficult behaviors. I have edited some of the text; please see the Table below for a summary of techniques, but please read through the article for an understanding of what you're doing and why. There is also a wonderful book: "SOS Help For Parents" by Dr Lynn Clark (see "recommended books" on our website, which can be found in the "Staying Healthy" section).
This article was taken mostly from the American Board of Pediatrics post on "Time Out" dated 7/26/2017:
Time-out (TO) is the most commonly employed tool for managing disruptive behavior and noncompliance in childhood. TO is well-supported by empirical evidence across a range of child populations, behaviors, and settings, and up to 85% of parents report having used the technique with their children. The use of time-out has been endorsed by the American Academy of Pediatrics (AAP). It is also supported by the Society for the Science of Clinical Psychology and the American Psychological Association. It should be noted, however, the implementation of this widely used technique continues to evoke controversy, fueled by the media and websites that often contain misinformation about possible negative consequences of TO.
By definition, TO (also known as social exclusion) is a form of behavioral modification that involves temporarily separating a child from an environment where unacceptable behavior is occurring. The concept of TO goes back almost 70 years and was promulgated by Arthur Staats, who used his own experiences with his 2 year-old daughter to establish much of what we now know of as TO. TO came into wide use beginning in the 1970s.
TO is usually applied to one of three situations: the presence of inappropriate behavior (eg, aggression or noncompliance), the presence of safety issues associated with the behavior (eg, child hitting others), and when the use of positive reinforcements by the caregiver have been ineffective due to the presence of other negative reinforcers in the child’s environment (eg, other children laughing at the behavior in a classroom setting). While there is a shortage of solid research on each of the specific variables within the TO technique, the success of TO overall has been empirically demonstrated. Key elements of TO include: the provision of an enriched, positive environment for the child not in TO; giving no more than one verbal warning to the child; delivering TO immediately following misbehavior; locating TO in a space with little or no reinforcement (such as toys, books, electronic equipment, etc); having a “backup” consequence if a child escapes TO; releasing a child from TO only when they have become calm; taking time to reinforce the reason why TO has occurred following the TO period (not while in it); and being consistent from one TO episode to another.
It is important to recognize that TO is effective only when there is a distinct contrast between the child’s normally positive and pleasurable activities (often called “time-in”) and the experience the child will have in TO. Time-in refers to the provision of a regular environment that is dense with reinforcement (eg, a high ratio of positive to negative interaction, physical affection, and activities of interest to the child). Also, the effectiveness of TO is clearly impacted by the amount of stimuli and activity available to the child during TO. The more social and visual interaction during TO (eg, someone looking at or talking with the child), the less effective TO becomes. As an aside, children who live in a home deprived of a rich and positive childhood experience (absence of good time-in) are less likely to respond to TO.
The success of TO has consistently been shown to have an inverse relationship with the length of time to the implementation of TO once warning of bad behavior has been given. Providing children with a single brief warning such as, “If you do not do as I say, you will go to TO,” does not decrease the efficacy of TO, but providing more than one warning does decrease the probable effectiveness of TO and does not reduce the number of subsequent TOs.
Evidence indicates that TO is significantly less effective if the child is allowed to determine when TO ends (eg, when they are “ready to leave”), compared to when an adult determines when TO is over. Research on the criteria for leaving TO indicates that contingent release (ie, releasing a child from TO only after a demonstrated period of quiet and calm behavior) is more effective in reducing disruptive behaviors and noncompliance compared with non-contingent release (eg, releasing a child after a period of time has elapsed regardless of the behavior at the time of release). Following release from TO, it is important to briefly discuss what has happened and why. Regarding noncompliant behavior, when TO is over, it is also important that the original command that got the youngster into TO is reissued quickly. For example, a child may refuse to comply with a parent's command to pick up his or her toys, because he or she finds the task to be unpleasant. If the child is placed in TO and is then not required to pick up the toys, noncompliance will be more likely in the future.
An important aspect of TO is its duration. TOs of moderate duration (approximately 4–5 minutes) are generally more effective than TOs of shorter or significantly longer duration, although the child’s age may influence this approach. The recommendation most often provided is that the length of time the child remains in time-out should correlate with the child's age - each year of the child's age constitutes 1 minute of TO. This is considered appropriate up to the age of 7 or so when time out starts to become less effective as a behavioral modifier.
The earliest age at which TO can be successfully implemented obviously depends on a toddler or older child’s ability to understand what he or she is being told and the child’s ability to respond. Some believe that TO can be started for some infants as early as a year of age. The Australian Association for Infant Mental Health has taken the position, however, that TO should not be used for children under the age of 3 years. It states that children younger than 3 years may not have the developmental capacity to make the connection between their behavior and the response of the caregiver. There are numerous parenting websites that advocate against the use of TO at any age.
The most common “errors” parents make included giving multiple warnings, talking to the child during TO, allowing access to interesting stimuli (eg, toys, books, electronics), and allowing visual access to other people while in TO. Parents who found TO as effective were significantly more likely to report delivering a single warning, providing a reason for the necessity of TO prior to or after (but not during) TO, and requiring the child to be calm prior to ending TO, rather than following a strict duration of TO. For parents who use TO, it is important that it be used correctly. Failure to see good results may cause some parents to conclude that TO is ineffective and then begin to resort to harsh methods of discipline, such as yelling or spanking.
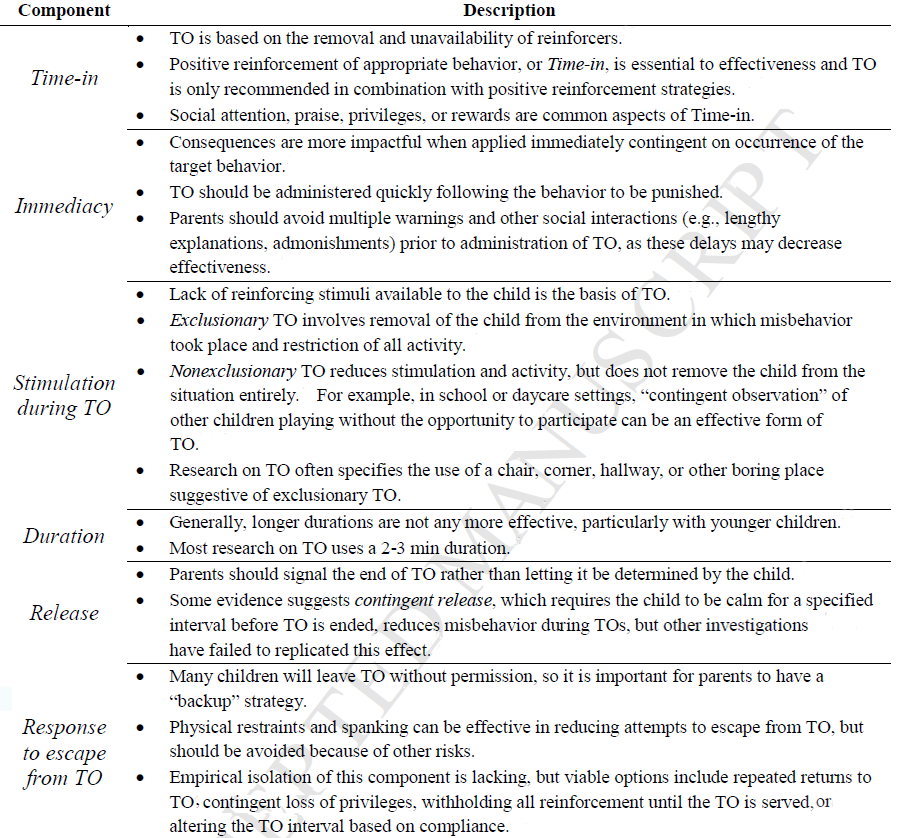
A summary of the key elements of TO appears in the Table below, which appeared in the Journal: Academic Pediatrics March 2017 Volume 17, Issue 2, Pages 168–175, "A Survey of Parents' Perceptions and Use of Time-out Compared to Empirical Evidence" David V. Wagner, PhD, Megan E. Tudor, PhD, Katharine E. Zuckerman, MD, MPH, Kurt A. Freeman, PhD, ABPP
Table
Key Components of Effective Time-out Administration
Contributed by Dr Brown:
Below is a great discussion on the "Time Out" Technique to control for difficult behaviors. I have edited some of the text; please see the Table below for a summary of techniques, but please read through the article for an understanding of what you're doing and why. There is also a wonderful book: "SOS Help For Parents" by Dr Lynn Clark (see "recommended books" on our website, which can be found in the "Staying Healthy" section).
This article was taken mostly from the American Board of Pediatrics post on "Time Out" dated 7/26/2017:
Time-out (TO) is the most commonly employed tool for managing disruptive behavior and noncompliance in childhood. TO is well-supported by empirical evidence across a range of child populations, behaviors, and settings, and up to 85% of parents report having used the technique with their children. The use of time-out has been endorsed by the American Academy of Pediatrics (AAP). It is also supported by the Society for the Science of Clinical Psychology and the American Psychological Association. It should be noted, however, the implementation of this widely used technique continues to evoke controversy, fueled by the media and websites that often contain misinformation about possible negative consequences of TO.
By definition, TO (also known as social exclusion) is a form of behavioral modification that involves temporarily separating a child from an environment where unacceptable behavior is occurring. The concept of TO goes back almost 70 years and was promulgated by Arthur Staats, who used his own experiences with his 2 year-old daughter to establish much of what we now know of as TO. TO came into wide use beginning in the 1970s.
TO is usually applied to one of three situations: the presence of inappropriate behavior (eg, aggression or noncompliance), the presence of safety issues associated with the behavior (eg, child hitting others), and when the use of positive reinforcements by the caregiver have been ineffective due to the presence of other negative reinforcers in the child’s environment (eg, other children laughing at the behavior in a classroom setting). While there is a shortage of solid research on each of the specific variables within the TO technique, the success of TO overall has been empirically demonstrated. Key elements of TO include: the provision of an enriched, positive environment for the child not in TO; giving no more than one verbal warning to the child; delivering TO immediately following misbehavior; locating TO in a space with little or no reinforcement (such as toys, books, electronic equipment, etc); having a “backup” consequence if a child escapes TO; releasing a child from TO only when they have become calm; taking time to reinforce the reason why TO has occurred following the TO period (not while in it); and being consistent from one TO episode to another.
It is important to recognize that TO is effective only when there is a distinct contrast between the child’s normally positive and pleasurable activities (often called “time-in”) and the experience the child will have in TO. Time-in refers to the provision of a regular environment that is dense with reinforcement (eg, a high ratio of positive to negative interaction, physical affection, and activities of interest to the child). Also, the effectiveness of TO is clearly impacted by the amount of stimuli and activity available to the child during TO. The more social and visual interaction during TO (eg, someone looking at or talking with the child), the less effective TO becomes. As an aside, children who live in a home deprived of a rich and positive childhood experience (absence of good time-in) are less likely to respond to TO.
The success of TO has consistently been shown to have an inverse relationship with the length of time to the implementation of TO once warning of bad behavior has been given. Providing children with a single brief warning such as, “If you do not do as I say, you will go to TO,” does not decrease the efficacy of TO, but providing more than one warning does decrease the probable effectiveness of TO and does not reduce the number of subsequent TOs.
Evidence indicates that TO is significantly less effective if the child is allowed to determine when TO ends (eg, when they are “ready to leave”), compared to when an adult determines when TO is over. Research on the criteria for leaving TO indicates that contingent release (ie, releasing a child from TO only after a demonstrated period of quiet and calm behavior) is more effective in reducing disruptive behaviors and noncompliance compared with non-contingent release (eg, releasing a child after a period of time has elapsed regardless of the behavior at the time of release). Following release from TO, it is important to briefly discuss what has happened and why. Regarding noncompliant behavior, when TO is over, it is also important that the original command that got the youngster into TO is reissued quickly. For example, a child may refuse to comply with a parent's command to pick up his or her toys, because he or she finds the task to be unpleasant. If the child is placed in TO and is then not required to pick up the toys, noncompliance will be more likely in the future.
An important aspect of TO is its duration. TOs of moderate duration (approximately 4–5 minutes) are generally more effective than TOs of shorter or significantly longer duration, although the child’s age may influence this approach. The recommendation most often provided is that the length of time the child remains in time-out should correlate with the child's age - each year of the child's age constitutes 1 minute of TO. This is considered appropriate up to the age of 7 or so when time out starts to become less effective as a behavioral modifier.
The earliest age at which TO can be successfully implemented obviously depends on a toddler or older child’s ability to understand what he or she is being told and the child’s ability to respond. Some believe that TO can be started for some infants as early as a year of age. The Australian Association for Infant Mental Health has taken the position, however, that TO should not be used for children under the age of 3 years. It states that children younger than 3 years may not have the developmental capacity to make the connection between their behavior and the response of the caregiver. There are numerous parenting websites that advocate against the use of TO at any age.
The most common “errors” parents make included giving multiple warnings, talking to the child during TO, allowing access to interesting stimuli (eg, toys, books, electronics), and allowing visual access to other people while in TO. Parents who found TO as effective were significantly more likely to report delivering a single warning, providing a reason for the necessity of TO prior to or after (but not during) TO, and requiring the child to be calm prior to ending TO, rather than following a strict duration of TO. For parents who use TO, it is important that it be used correctly. Failure to see good results may cause some parents to conclude that TO is ineffective and then begin to resort to harsh methods of discipline, such as yelling or spanking.
A summary of the key elements of TO appears in the Table below, which appeared in the Journal: Academic Pediatrics March 2017 Volume 17, Issue 2, Pages 168–175, "A Survey of Parents' Perceptions and Use of Time-out Compared to Empirical Evidence" David V. Wagner, PhD, Megan E. Tudor, PhD, Katharine E. Zuckerman, MD, MPH, Kurt A. Freeman, PhD, ABPP
Table
Key Components of Effective Time-out Administration